| # | Outside U.S. | U.S. (In Network) | U.S. (Outside Network) |
|---|---|---|---|
| Lifetime Maximum Benefit | Unlimited | Unlimited | Unlimited |
| Calendar Year Maximum Benefit | Unlimited | Unlimited | Unlimited |
| Preventive Care | You pay $0 | You pay 20% | You pay 40% |
| Primary Care | You pay $10 | You pay $30 | You pay 40% |
| Lab work & X-ray | After deductible, You pay $0 | After deductible, You pay 20% | After deductible, You pay 40% |
|---|---|---|---|
| Urgent Facility | You pay $0 | You pay $75 | You pay 40% |
| Emergency Room | After deductible, you pay $50 copayment | After deductilbe, you pay 20% and additional $50 copayment | After deductilbe, you pay 40% and additional $50 copayment |
| Ambulance | After deductible, you pay $0 | After deductible, you pay 20% | After dedutible, you pay 40% |
| Surgery | After deductible, you pay $0 | After deductible, you pay 20% | After dedutible, you pay 40% |
| Inpatient Service | After deductible, you pay $0 | After deductible, you pay 20% | After dedutible, you pay 40% |
| Prescription | Deductible is not applicable. 100% of the actual charge up to a Calendar Year maximum of $2,500 | Deductible is not applicable. 100% of the actual charge up to a Calendar Year maximum of $2,500 | Deductible is not applicable. 100% of the actual charge up to a Calendar Year maximum of $2,500 |
| Maternity Care/Obstetrical Services | Not Covered | Not Covered | Not Covered |
| Dental Care required due to an Injury | Maximum of $1,000 per Calendar Year, maximum/$200 per tooth | Maximum of $1,000 per Calendar Year, maximum/$200 per tooth | Maximum of $1,000 per Calendar Year, maximum/$200 per tooth |
| Plan detail information | |||
| Outside U.S. | |
|---|---|
| Lifetime Maximum Benefit | Unlimite |
| Calendar Year Maximum Benefit | Unlimited |
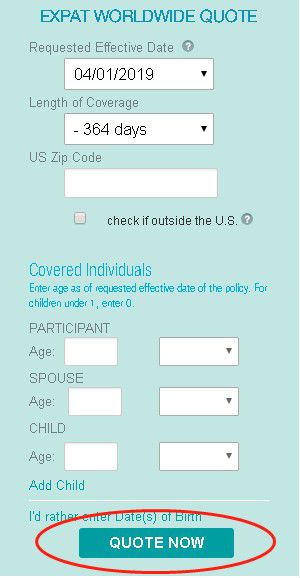
| Calendar Year Deductible | Option: $0, $2500, $5000, $10,000 |
| Preventive Care | You pay $0 |
| Primary Care | You pay $10 |
|---|---|
| Lab work & X-ray | After deductible, you pay $0 |
| Urgent Facility | You pay $0 |
| Emergency Room | After deductible, you pay $0 |
| Ambulance | After deductible, you pay $0 |
| Surgery | After deductible, you pay $0 |
| Inpatient Service | After deductible, you pay $0 |
| Prescription | Deductible is not applicable. 100% of the actual charge up to a Calendar Year maximum of $2,500 |
| Maternity Care/Obstetrical Services | Not Covered |
| Plan detail information |
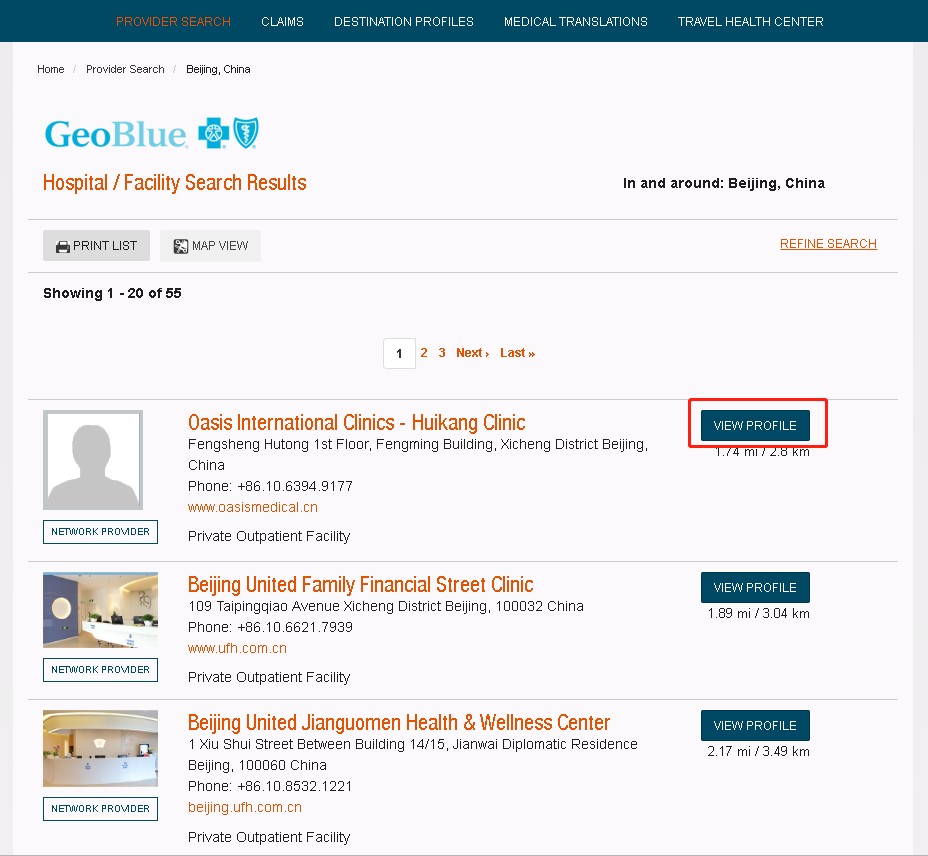
| Beijing |
|---|
| Beijing United Family Healtdcare |
| Beijing Oasis International Hospital |
| Beijing 21st Century Hospital |
| Beijing New Century Children's Hospital |
| Beijing Bayley & Jackson Medical Center |
| International Medical Center - Beijing |
| Beijing Vista Medical Center |
| Mary's Hospital for Women & Infants |
| Hong Kong International Medical Clinic, Beijing |
| Shanghai |
|---|
| Shanghai Delta West Clinic |
| Yosemite Clinic |
| Shanghai United Family Hospital(Pu Dong/Chang Ning) |
| Shanghai Concord Medical Cancer Center |
| Guangzhou |
|---|
| Guangzhou United Family Hospital |
| Eur Am International Medical Center |
| Chang Jiang International Medical Center |
| Nanfang Hospital Affiliated to Nanfang Medical University |
| Hong Kong |
|---|
| Queen Elizabeth Hospital |
| Quality HealthCare Medical Centre |
| Human Health Medical Centre |
| Taiwan |
|---|
| Wan Fang Hospital |
| Linkou Chang Gung Memorial Hospital |
| Taoyuan Chang Gung Memorial Hospital |
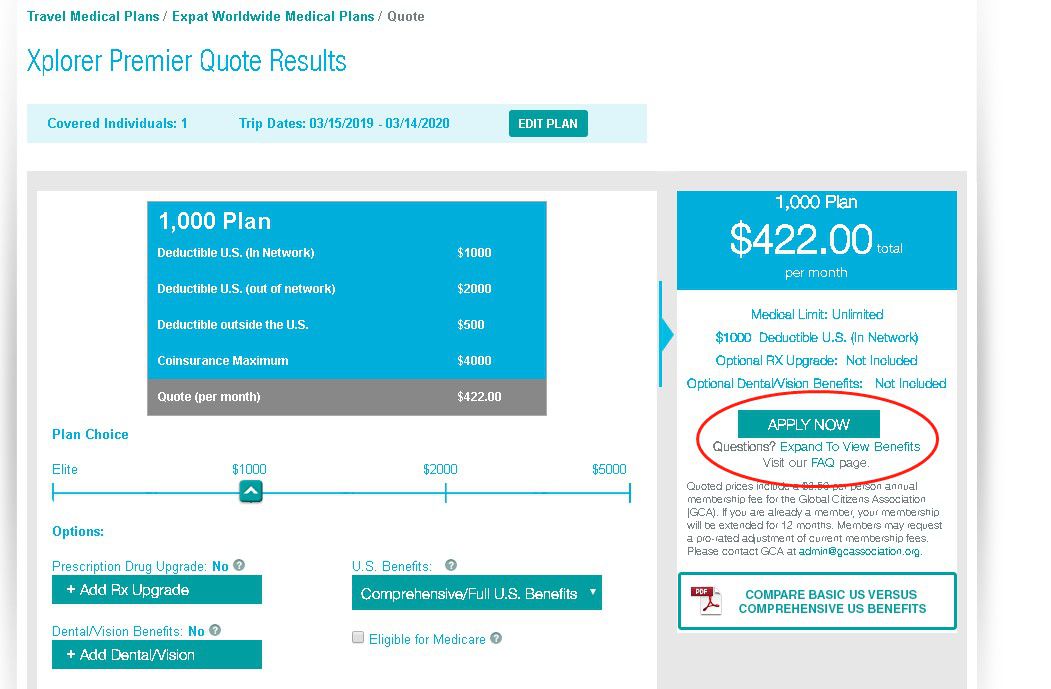
| Annual Deductible | Outside U.S. | Inside U.S. (In-Network) |
Inside U.S.(Out-of-Network) | Coinsurance |
|---|---|---|---|---|
| $0 | $0 | $0 | $1,000 | $2,000 |
| $1,000 | $500 | $1,000 | $2,000 | $4,000 |
| $2,000 | $1,000 | $2,000 | $4,000 | $8,000 |
| $5,000 | $2,500 | $5,000 | $10,000 | $10,000 |
| Deductible | Outside U.S. | Inside U.S. (In-Network) |
Inside U.S.(Out-Network) | Coinsurance |
|---|---|---|---|---|
| $0 | $0 | N/A | N/A | $2,000 |
| $1,000 | $1,000 | N/A | N/A | $8,000 |
| $2,500 | $2,500 | N/A | N/A | $10,000 |
| $5,000 | $5,000 | N/A | N/A | $10,000 |